What food would you say is your specialty?
Chile and pan cakes… Flap jacks, baked alaska and impossible pie
Festivals, death, suicide, Drumming, Fire Keeping, Spirituality, Pagan, Paganism, Brighid,
What food would you say is your specialty?
Chile and pan cakes… Flap jacks, baked alaska and impossible pie
What have you been putting off doing? Why?
Way to many things.
The facilitator for this course attempted to nab me on plagiarism for this assignment as I used a generative AI to produce it. This annoyed me as a/ I did not sign up for an intro to psych course to become a content creator.
Here is the file that almost cost me my course
What was the hardest personal goal you’ve set for yourself?
Starting my own business.
Who are your favorite artists?
Me please see
According to the American Psychiatric Association, the DSM-5-TR or Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision is an assistive written text used by healthcare professionals to aid or facilitate in the diagnostic process of determining whether or not a condition exists given a set of criterion as specified by the manual1.
The Manual itself originally started life as “The American Medical Association’s Standard Classified Nomenclature of Disease “ in 19172 Furthermore, it has gone through several iterations and naming conventions until its present-day name of the DSM-5-TR hereto shall be referred to as “The DSM” for simplicity.
The DSM has three major components:
I cannot really express more than what I have already expressed in a previously written work, so I shall just re-iterate what I have already said
For over ten years, I worked as a technical support specialist in a call center and seven years as a field service technician for a small wireless internet service provider. As a Diagnostician, I have seventeen years of experience if I combine the knowledge from those two jobs. The jobs involved troubleshooting cell phones, computers, network infrastructure, and people.
Over that time, several colleagues and I attempted to write a Troubleshooting manual for computer, cell phone, and network-related issues; oh yes, and let’s remember people. Have You seen our book? No, you have not; why is this? There were many attempts, but the book never made it off the many pages written. The reasons for this were simple: the possible scenarios were too numerous, and the classification of issues became too cumbersome on cross reference, as were the potential fixes. In short, the unwritten book to help fix the broken became broken. It was too complex in its working and lacked fluidity; it in itself lacked the reasoning power of the Human Brain. And then there was a need for future updates. Yes, the book idea broke.
In walks the DSM, a diagnostic aid for. Wait one minute; please see the previous paragraph.
In addition to this, one may want to look at more scholarly works where issues are identified with measuring psychiatric illness. I will reference in particular, here the determination of ADHD utilizing the E-Swan test, which is a questionnaire utilized in diagnosing ADHD based on the criteria set out within the DSM IV and DSM-5. Both the papers listed below express issues with the wording utilized within the questionnaires, and both list potential issues with comprehension of the test by its recipients. How can The DSM set out the criterion for determining a condition if definitive, accurate tests cannot be established to satisfy its specification? Is the problem the test, The DSM’s criterion, or both?
Blume, F., Buhr, L., Kuehnhausen, J., Köpke, R., Weber, L. A., Fallgatter, A. J., … Gawrilow, C. (2020, June 25). Validation of a Self-Report Version of the German Strengths and Weaknesses of ADHD Symptoms
Normal Behavior Scale (SWAN-DE-SB). https://doi.org/10.31234/osf.io/x6bpd and Alexander, L.M., Salum, G.A., Swanson, J.M. and Milham, M.P. (2020), Measuring strengths and weaknesses in dimensional psychiatry. J Child Psychol Psychiatr, 61: 40-50. https://doi.org/10.1111/jcpp.13104
1https://www.psychiatry.org/psychiatrists/practice/dsm/about-dsm
2https://www.psychiatry.org/psychiatrists/practice/dsm/about-dsm/history-of-the-dsm
In attempting to define what is Abnormal Behaviour the first thing that comes to mind is an axiom of Sherlock Homes “When you have eliminated the impossible, whatever remains, however improbable, must be the truth.—Arthur Conan Doyle (author, 1859–1930, in “The Sign of Four”).” In the case of Abnormality, we must first understand what is normal, and whatever else remains becomes abnormal. Concerning the Homes axiom, it is interesting that people attribute deductive reasoning to his sleuthing skills; however, he utilizes inductive reasoning. Homes further states, “It is a capital mistake to theorize before you have all the evidence. It biases the judgment. —Arthur Conan Doyle (in “A Scandal in Bohemia”).” Deductive reasoning follows the scientific method, meaning it begins with a hypothesis, examines facts, and, from the findings, reaches a logical conclusion that either proves or disproves the stated hypothesis. However, I believe the best approach is to utilize Inductive reasoning when one seeks to understand Abnormality. With my understanding of both methods, deductive reasoning begins with a preconceived statement that needs to be proved or disproved and can be biased. In contrast, Inductive reasoning starts with a question and sets out to answer that question with no preconceptions as to whether or not it is proper to conclude.
The DSM-5 defines abnormal behavior as “behavior characterized by one or more of the following four criteria: maladaptive behavior, personal distress, statistical rarity, and violation of social norms.Jul 24, 2023”
Maladaptive behavior is characterized as things that prevent an individual from functioning normally within Society and may cause the individual to harm others or themselves. Things such as withdrawal from social situations, outbursts of anger that are uncharacteristic of social norms. Substance abuse as a coping mechanism. 1
Personal distress While similar to maladaptive behavior it is more self-centric; feelings of worry, anxiety, or discomfort are focused on the self without referencing how their behavior may affect others.2
Statistical rarity in clinical terms is the needle in the haystack so to speak. The zebra in a field of horses. This probably is one of the more important determining factors of what is abnormal behavior A Rarity looks at the overall norms of Society as a whole to determine whether or not the behaviour fits within the whole societal set. 3
Violation of social norms goes hand and hand with statistical rarity but sometimes may cause a false positive as the data set looked at may be too small. In a true determination, we must look at the Macrocosm, not the microcosm. In other words, Society as a whole vs. a cultural subset of the world society.
Several key groups are instrumental in diagnosing and treating abnormal behaviors. Amongst them psychiatrists, clinical psychologists, and social workers. The team is not limited to just these three groups, but for the purpose of this paper, we will focus on them for now.
Social workers are sometimes the front of the line, or near front of the line. Although they may not have the ability to make a diagnosis of a condition, they may encounter it before an individual ever encounters a psychiatrist or clinical psychologist. Their role in treatment may begin with Identifying an issue, holding individual counseling sessions, setting up peer groups, referrals to health professionals: psychologists et al. le, acting as a liaison between organizations, assisting with setting up treatment plans, and many other things. 5
Psychiatrists have three main roles: first, to assess the individual and diagnose whether or not a condition exists; if one does, then develop a treatment plan that aims to help the individual incorporate new strategies and coping mechanisms that allow the individual to function within Society. Lastly, ongoing care to ensure that the individual continues on a beneficial path. 6
Clinical psychologists are more academic in their approach. They study individuals who may be under the care of a psychiatrist or may experiment with the regime of care for the individual with the express intent of promoting change for the betterment of future care. 7
Issues and values around abnormal behaviors and mental illnesses.
When looking at mental illness and abnormal behaviors, there are a multitude of facets from which to look at the overall picture. And they most definitely exceed the scope of this limited work. Looking at Values, one can only hope the underlying premise is the betterment of Society and the individual as wholes or parts thereof. Historically, however, there were dark periods in the world of psychiatry. I would highly recommend reading “Asylums: Essays on the Social Situation of Mental Patients and Other Inmates” Erving Goffman, 1961 First Anchor Books. Goffman attempts to answer some of the questions pertaining to Stigmatisms associated with mental illness, the treatment process, the conditioning that occurs as a result of treatment in the closed societies of mental health wards, prisons and other such entities. Not only does Goffman look at things from the perspective of the patient or inmate, he also looks at the perspectives of the clinicians, the people assigned to keep order, and the administrations.
The DSM5 is a tribute to the advancement of the betterment of Society as a whole. Being an organic document it is being updated to reflect new findings, and removing old and incorrect data. Its only drawback I can see is that its ability to change sometimes is slower than it should be. One can hope that it becomes more adaptable with advancements in cloud technology.
Going back to issues surrounding abnormal behaviours and mental issues first and foremost is the stigmatism associated to it by Society itself or internally 8 the stigma alone stop many from being diagnosed and treated. Historically we have to look at incorrect assessments and beliefs such as being gay is a mental illness9 This is one instance where the DSM took far too long to update. The initial vote to remove this category from the DSM was in 1973, and it passed that it be removed; it took nearly 14 years, 1987 to be exact, until it was removed in totality. So for 14 years the possibility for incorrect treatment existed.
In short, I have exhausted the scope of this assignment, for I fear that if I continue to delve into it, it may become a thesis.
1https://www.medicalnewstoday.com/articles/maladaptive-behavior#types
2https://academic-accelerator.com/encyclopedia/personal-distress
3https://psychologycampus.com/abnormal-psychology-behaviors-that-lay-outside-the-norm/
4https://psychologycampus.com/abnormal-psychology-behaviors-that-lay-outside-the-norm/
5https://www.casw-acts.ca/en/social-work-practice-mental-health
6https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3410123/#:~:text=Overall%2C%20psychologists%20assess%2C%20diagnose%2C,to%20physical%20and%20mental%20health.
7https://www.apa.org/education-career/guide/subfields/clinical
8https://www.youtube.com/watch?v=lXYP3kdWSEw
9https://www.psychologytoday.com/ca/blog/hide-and-seek/201509/when-homosexuality-stopped-being-a-mental-disorder
I am not going to touch on the DSM directly here. However, I do have some cross-experience in a seemingly unrelated field, but is it?
For over ten years, I worked as a technical support specialist in a call center and seven years as a field service technician for a small wireless internet service provider. As a Diagnostician, I have seventeen years of experience if I combine the knowledge from those two jobs. The jobs involved troubleshooting cell phones, computers, network infrastructure, and people.
Over that time, several colleagues and I attempted to write a Troubleshooting manual for computer, cell phone, and network-related issues; oh yes, and let’s remember people. Have You seen our book? No, you have not; why is this? There were many attempts, but the book never made it off the many pages written. The reasons for this were simple: the possible scenarios were too numerous, and the classification of issues became too cumbersome on cross reference, as were the potential fixes. In short, the unwritten book to help fix the broken became broken. It was too complex in its working and lacked fluidity; it in itself lacked the reasoning power of the Human Brain. And then there was a need for future updates. Yes, the book idea broke.
In walks the DSM, a diagnostic aid for. Wait one minute; please see the previous paragraph.
What’s your favorite recipe?
Actually read any of these posts or am i just being trolled by a bunch of bots?
If you are actually reading the posts, and are subscribed why are none of you clicking on any of the other posts i make?
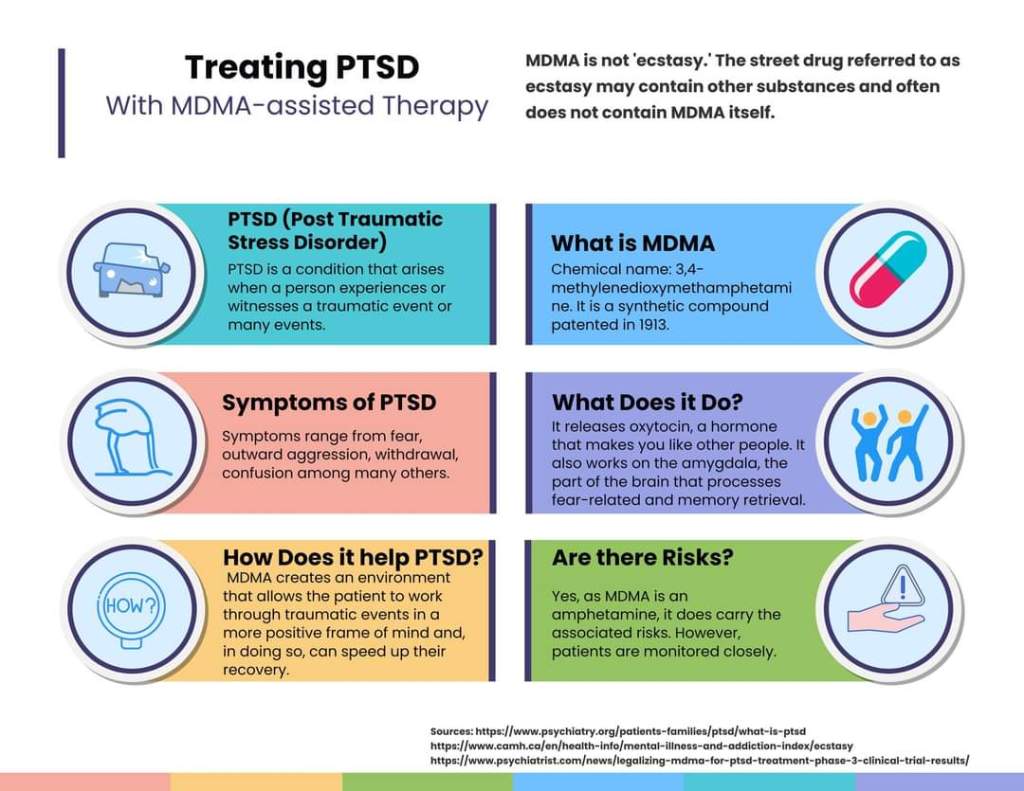
This is an infographic I did recently for my psych class. Therapists have been using MDMA as a tool to help PTSD sufferers recover from this deblitating condition, it is in trials and legalization of this drug for the purpose full on treatment is in the works.